We value your privacy
We use cookies to enhance your browsing experience, serve personalized ads or content, and analyze our traffic. By clicking "Accept All", you consent to our use of cookies.
We use cookies to help you navigate efficiently and perform certain functions. You will find detailed information about all cookies under each consent category below.
The cookies that are categorized as "Necessary" are stored on your browser as they are essential for enabling the basic functionalities of the site. ...
Necessary cookies are required to enable the basic features of this site, such as providing secure log-in or adjusting your consent preferences. These cookies do not store any personally identifiable data.
No cookies to display.
Functional cookies help perform certain functionalities like sharing the content of the website on social media platforms, collecting feedback, and other third-party features.
No cookies to display.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics such as the number of visitors, bounce rate, traffic source, etc.
No cookies to display.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
No cookies to display.
Advertisement cookies are used to provide visitors with customized advertisements based on the pages you visited previously and to analyze the effectiveness of the ad campaigns.
No cookies to display.

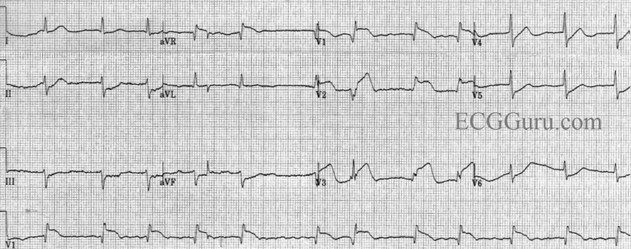
This is an acute anterior epicardial ischemia – also known as an acute anterior MI. We used to call it an anteroseptal MI but today we call it an anteroapical MI. That’s because the proximal septum is not usually involved in these infarctions. Instead, it is the lower septum and the adjacent apical myocardium that is involved.
The first site of ventricular depolarization is just distal to the mid-septum. Depolarization then proceeds throughout the rest of the left ventricle in a counterclockwise manner with the proximal (basilar) septum being among the last areas of the left ventricle to be activated.
But what is so interesting about this particular myocardial infarction? Let’s look closer…
This is a left anterior descending (LAD) artery occlusion that has occurred proximal to the first septal perforator. How do I know that? How can you determine the level of occlusion of the LAD?
To understand how to do that, we must recall some very basic (and schematic) anatomy of the left anterior descending artery.
When we visualize the LAD artery, we aren’t thinking of an “anatomically-correct” diagram; instead, we think of a schematic, conceptualized picture, like this:

Usually, the first branch from the LAD is the first septal perforator (Fig. 2). Actually, there are more septal perforators, but we are only interested in the first one. It will serve to represent all the septal perforator branches. The septal perforators extend into the interventricular septum perpendicular to the LAD and provide circulation to the upper 2/3 of the septum.
Usually, the second branch from the LAD is the first diagonal branch. Actually, there are anywhere from two to four diagonal branches of varying lengths (and occasionally, even one or two more) which course down the lateral surface of the left ventricle… but we are only interested in the first one. It will serve to represent all the diagonal branches.
In most people, the first septal perforator is the first branch off the LAD, followed closely by the first diagonal branch (Fig. 2). Very infrequently, the first diagonal branch is the first branch off the LAD (Fig. 2-B), followed very closely by the first septal perforator branch.
You will often hear discussions of whether there is a proximal or distal occlusion of the LAD. When the word proximal is used in this context without mentioning “proximal to what?” it is assumed proximal (or distal) to the first diagonal branch – not the first septal perforator.
Let’s begin by learning how to ascertain if the occlusion is proximal or distal to the first diagonal branch…
1.
The first thing to be done is to ascertain whether the occlusion actually involves the LAD. ST elevation in V1 – V3 without concurrent STE in the inferior leads is a good sign that the occlusion is indeed occurring in the LAD. The left circumflex artery (LCx) does not reach the area of Leads V1 and V2 and the RCA would very, very rarely cause ST elevation in Leads V1 and V2 without concurrent ST elevation in the inferior leads.
OK… now where in the LAD is the occlusion located?
2.
To determine if the occlusion is proximal to the first diagonal branch, look at the ST segments in Leads II, III and aVF (the inferior leads). If they all have depressed ST segments, the occlusion is proximal to the first diagonal branch. In this ECG, the occlusion is proximal to the first diagonal branch. If there were no ST depression in the inferior leads, the occlusion would be distal to the first diagonal branch.
OK… we’ve determined that this LAD occlusion is proximal – proximal, that is, to the first diagonal branch. But how can we determine whether the occlusion is proximal or distal to the first septal perforator?
3.
First, look at Leads aVR and V1. If there is ST elevation in both leads, then the occlusion is proximal to the first septal perforator. But if neither lead manifests ST elevation – or, if there is ST elevation in one lead but not the other – then we cannot say with certainty that the occlusion is proximal to the first septal perforator based on that criterion. But don’t give up yet! We have one more card up our sleeve: if there is ST depression in Lead V6, then the LAD occlusion is proximal to the first septal perforator.
So, while there is only ONE criterion for determining the location of the occlusion with respect to the first diagonal branch (ST depression in the inferior leads), there are two criteria for determining the location of the occlusion with respect to the first septal perforator. The occlusion on this ECG is proximal to the first septal perforator.
Why is this information important? It’s the difference between reading and interpreting an ECG! Reading the ECG establishes the presence of an acute STEMI in the LAD. Interpretation is knowing that the occlusion is proximal to the first diagonal branch, alerting you to the fact that this is a STEMI with a very large area at risk. The larger the area at risk, the greater the likelihood of a decreased ejection fraction and cardiogenic shock! The larger the area at risk, the greater the likelihood of a paroxysmal polymorphic ventricular tachycardia appearing during the very early stages of the ischemia. Let me translate that for you: All this while still under your care!
If the occlusion is proximal to the first septal perforator the right bundle branch may become blocked acutely, leading to an acute, dyssynchronous contraction of the ventricles – at the worst possible time! This adds an additional negative factor to the likelihood of a reduced left ventricular ejection fraction and a lethal cardiac tachydysrhythmia – again, all while under your watch!
Beginners read ECGs…
…professionals interpret them!
In Part 2, you will learn why this particular ECG may be much more ominous than you suspect even now!
Notifications